Okay, this has bugged me a little bit and I had to write a post as a comment on what I have seen. I have previously commented on some of the research that has come out over the last few years suggesting that - to coin a sensationalist media-friendly phrase - Marathon Running Is Bad For Your Heart. I recently saw this TED talk from Dr. James O'Keefe M.D., where he discusses many of the same ideas. As a cardiologist, he used to exercise regularly as the generally accepted standpoint is that exercise is good for your heart, and the more the better. But he and his colleagues have since found that over-intensive running may in fact be bad for your heart. Instead we should all be running not too fast and not too far.
Now, as an ultramarathon runner, I am obviously biased in my opinions. However, I do know a fair bit about data analysis and (more importantly) interpretation. And based on what I have seen in the literature, I have yet to see anything that makes me particularly worried.
So let's have a play-by-play of the content of the video. Granted, the point of TED talks is to make a complex subject understandable by non-experts so this isn't a scientific presentation as such, but in this presentation you can see issues with the argument. I apologise for how long this post is, but I want to be thorough in my assessment. I do not claim to be an expert in the area of cardiology, and I certainly haven't read all of the literature (I just do this in my spare time for fun after all), but nothing that I have seen in these studies has suggested anything more than one possible interpretation of the data.
One of the first examples of problems with long distance running that is brought up is the story of Pheidippides, the Greek herald who ran the 26 miles from Marathon to Athens to proclaim victory against the Persians, whereupon he promptly fell down dead. How could a human possibly run so far without his heart giving in? Well, of course we know that it is quite easy - thousands of people do it every year. There is evidence that it is our ability to run long distances that set us apart from other animals and allowed us to become the dominant species on earth. What Dr. O'Keefe fails to mention is that other versions of the Pheidippides story have him running from Athens to Sparta and back again the day before (~300 miles). It may potentially be nothing more than a myth, but we know that human beings are more than capable of such feats of endurance (James Adams and Mimi Anderson will be doing it later this year) so it's not beyond the realms of possibility. I don't claim that such distances are sensible by any means, but when he talks about "running far", I just think that we need to have a little perspective on what "far" really means.
Dr. O' Keefe also goes on to mention the fact that there are actually very few deaths in marathons (fewer than 1 in 100,000 runners die), which sort of goes against his whole thesis. Of those that have unfortunately passed away during marathons, most are due to hyponatremia due to over-drinking and are nothing to do with cardiovascular problems. Of those that are due to cardiovascular problems, it is not obvious how many were underlying problems exacerbated (but not caused by) running, or by the runner attempting an endurance event that they had not properly trained for.
He discusses the urban myth that marathon running makes you immune from heart attacks. Yep, I agree that that is utter rubbish. Does that mean that running marathons causes heart attacks though?
We see an example of one of Dr. O'Keefe's friends, John, who has been running 12 miles or more a day for the last 45 years. We see a CT scan showing the difference between John's heart and that of a "normal" person. This scan shows calcium deposits in the heart, with a score over 100 suggesting a mild increased risk of a cardiac event, and a score over 1,000 suggesting a high risk. It is clear that there is severe calcification in the coronary artery, but the question is; is this down to his running? John is nearly 70 years old, so it's fairly likely that he would show a non-normal coronary artery calcium (CAC) level. This study by the American Heart Association (based on 6,110 individuals) shows that a caucasian male of 70 years old has a roughly 80% chance of having a CAC above normal (Figure 1B). John's CAC count sits pretty much bang on the 90th percentile of caucasian males (Figure 3), so his count is definitely high, but claiming that it is due to running is quite a leap. You could say that his running didn't prevent it (which goes back to the point above), but another way of looking at it is that he hasn't had a heart attack despite having high calcification in the heart. I'm not saying that running wasn't to blame for the calcification, but finding an individual (N=1) who is a runner and also has high CAC levels does not prove that. Correlation does not prove causation.
This one really bugged me, and is the reason I decided to write this post. We see a figure showing the reduction in all-cause mortality rates versus the length of exercise for 416,175 Taiwanese (not Chinese as the video suggests) individuals (let's ignore the fact that there are HUGE differences in cardiac rates between different ethnic groups). This figure is shown in Dr. O'Keefe's 2011 review paper in the Mayo Clinic Proceedings Journal "Potential Adverse Cardiovascular Effects from Excessive Endurance Exercise". You can see the figure here. The original paper from The Lancet can be found here. Here's what this figure says to me:
- Daily exercise results in a reduction in mortality rates
- Doing vigorous exercise is better than doing moderate exercise
- The benefits that you get for exercise plateau (no shit - so we can't just keep exercising and NEVER DIE?!)
- You hit the plateau sooner with vigorous exercise than with moderate exercise (~1 hour vs ~2 hours)
- But this is the crucial one - the plateau for vigorous exercise is still considerably higher than for moderate exercise (~45% vs ~30%)
Next we see Darwinian evolutionary theory brought into play. "Charles Darwin was wrong about one thing though; it's not survival of the fittest, it's the survival of the moderately fit". I'm going to give the benefit of the doubt here, and assume that this is just for the sound-bite. But I hope that everybody is aware that the suggestion that physical fitness is the driving force for natural selection is a misnomer. Fitness is a measure of the adaptability of an organism to its local environment. The phrase itself was not even devised by Darwin in his initial On the Origin of Species, but was coined by Herbert Spencer.
Next up we see a figure showing that cardiac death rates go down as exercise intensity and longevity increases, but that the reduction in mortality plateaus. So? How does he get from that to "Too much = Harm"?
Okay, now we're getting a bit more into things. How does running result in problems with the heart? Obviously running (or any form of vigorous exercise) results in a massive increase in blood flow, and the heart muscle has to pump harder to supply the increased oxygen levels required to the muscles. As mentioned, various studies have been performed measuring cardiac troponin levels (Troponin T and I), and typically show that an appreciable number of marathon runners (in some cases up to half, in others much fewer) have elevated levels. For instance, here is one from the Journal of the American College of Cardiology (JACC), another from the Annals of Emergency Medicine (AEM) looking at runners of the Boston Marathon, and one looking at runners of the Perth marathon from the Medical Journal of Australia (MJA).
There's certainly no doubt that these studies suggest that intense physical activity results in the release of cardiac Troponin as the cardiac muscles contract and tear. However, what is not mentioned is that after the race, these runners' hearts returned to normal function, and in fact that the runners' normal function is better than non-runners (i.e. a lower heart rate). Cardiologist Dr. Malissa J. Wood M.D. (one of the authors of the JACC study) has said in a Runners' World article that she felt that the various studies were misinterpreted, and makes a very good point that the runners that they studied at the Boston marathon were all healthy despite the troponin leaks. It is the same as any muscle - it hurts like hell when you run and the muscles break down, but they quickly get rebuilt stronger than ever. One thing that they found was that training had a huge effect on the levels of troponin - those people in the study who were doing the most training saw the least troponin leakage.
So the point isn't that running marathons is bad for your heart, but rather that running marathons without training properly for it is bad. If you regularly train your heart, it gets stronger. Also interestingly in the JACC report, they report that "there was a higher incidence of post-exercise cardiac Troponin in marathon-type events in contrast to ultra-marathon competitions", and in fact the shorter (and hence more intense) the race, the higher the troponin levels. So the idea that the further you go the worse it is for your heart seems completely at odds with the research. It is in fact the intensity that results in the cardiac damage, but whether this damage is anything to worry about or merely the body's way of building up the heart is another question. The number of people that regularly compete in marathons and the like every year without their hearts bursting suggests the latter. Dr Wood's conclusion is:
"There are no data to suggest that there are long-term sequelae to the increase in biomarkers and echocardiographic evidence of injury in this setting. In contrast, many studies suggest that endurance exercise is associated with a reduction in cardiovascular risk and an increased life expectancy."
Now we start to move into some of the research conducted by LeGerche et al ("Exercise-induced right ventricular dysfunction and structural remodelling in endurance athletes") which shows that ultra-endurance events result in a decrease in right ventricular (RV) function, leading to a reduction in deoxygenated blood flow to the lungs. I have already looked at what I consider to be methodological flaws in this paper here, and remain unconvinced that these data represent a valid reason to stop running. Generally, the athletes showed a reduction in RV function during their respective races and this is what Dr. O'Keefe describes here. However, if you read the paper, you see that RV function returns to normal after the race. Also, the reduction in RV function is very low for marathon runners and not even (in my opinion) statistically significant. For Iron Man triathletes it is much more appreciable (because it is the longest event - it would be interesting to see similar results for ultramarathon runners), but RV function still returns to normal post race. As with the troponin levels, this suggests that your heart is put under immense strain when you exercise (big surprise), but importantly it returns to normal afterwards (and given the reduced heart rate of many runners it actually gets better than normal).
Of the 40 people studied (of which only 7 were marathon runners, the rest being cyclists or triathletes), 5 showed more serious evidence of chronic fibrosis in the interventricular septum. How many of these were runners is not clear, but it is likely that the majority (if not all) of these 5 were from the non-marathon group. It is presented to us as what happens in these veteran athletes, as their heart becomes "old before its time". First of all, it is only observable in 12.5% of a small cohort of athletes, and there could be any number of reasons behind it. Also, these athletes were the older and hence more experienced of the athletes. You could read this as "the athletes that have competed for the longest show this issue, hence it is a problem with training", or alternatively "the older athletes show this issue, hence it is a problem with age". These athletes were generally slightly older than the athletes that showed no signs of fibrosis (although the difference was not statistically significant), but had generally been competing for longer, so it is possible that this suggests an increased prevalence of this form of cardiac fibrosis in runners who had been training for longer. But the sample size is so small that it is difficult to ascertain such a thing without further investigation. If we took a random subset of 40 age-matched non-athletes, how many would show cardiac fibrosis I wonder?
Dr. O'Keefe next mentions a paper along these lines showing that runners show 62% more coronary plaques than sedentary people, and that this has been replicated. I cannot find the first paper, but the replicate paper is this study, published in the European Heart Journal. 108 male Masters marathon runners over 50 who have competed in more than 5 marathons in the previous 3 years were considered, and were matched up either by age (group II) or by age and other risk factors such as BMI, smoking status, etc. (group III) to a group of sedentary individuals. It is clear that blood pressure and heart rate are lower for marathon runners than for the control groups, but what they weren't expecting was that higher CAC levels were seen more often in marathon runners than in group III controls (but not when compared to group II controls). The conclusion of the study is:
"Regular marathon running has a beneficial effect on the cardiovascular risk factor profile but the extent of calcified coronary plaque is
underestimated from that risk factor profile, with 36% of marathon
runners aged >50 having a CAC score >100 and 9% of these
requiring coronary revascularization during two years of follow-up.
Advanced CAC scores seem to contribute to increased myocardial
damage and appear to impair outcome. Frequent marathon running
may not protect these athletes from the risk of coronary events. "
Edit (this paragraph was missed out in the original post): During about 2 years of follow up, 4 of the runners suffered from cardiac events, but there is unfortunately no similar count for the control samples (although the evidence notes that these numbers are "in a similar magnitude, though, as previously reported from other asymptomatic low-risk cohorts". This analysis is certainly the best evidence that I have seen so far to support the claim that running may actually cause problems with the heart, but there are certainly alternative explanations. The method for matching the controls in group III in particular may bias the results. After all, what the comparison with this group says is that "running marathons results in no significant change in CAC levels but does give a huge benefit to various other risk factors for cardiac disease (lower chance of stroke, lower risk of diabetes, lower Framingham risk score, lower cholesterol, lower risk of hypertension, lower blood pressure, lower heart rate, lower BMI, etc.), but if we ignore all of those then running puts you more at risk of a cardiac problem". Hmm. Does that seem a little unfair to anybody else? Also, there was a high level of selection bias in the marathon runner cohort, as the runners who put themselves in for such a test may be people more worried about their health to begin with as this Editorial response to the original paper suggests. Note for instance that more than 50% of runners were former smokers - this suggests that this cohort does not represent a truly accurate sub-population of marathon runners. It is possible that the majority of these runners were in fact people who had taken up running relatively late in life to correct for poor health choices earlier in their lives.
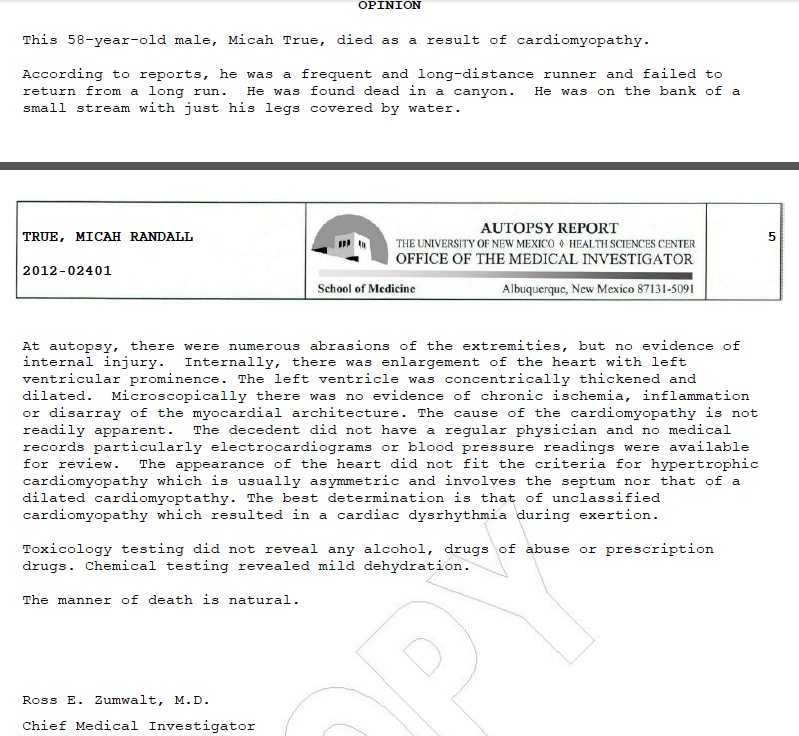
Next up we see a reflection on the death of Micah True, the legendary runner from Christopher McDougal's Born To Run, who unfortunately died last year at the young age of 58 whilst out on a routine training run. I was lucky enough to meet Micah last year, and he was a very friendly and unassuming individual. He ran because he loved to run, and had no agenda having had fame thrust upon him. He didn't care about arguments of barefoot vs shod running (for the record, he and the Tarahumara Indians do not run barefoot). He just loved to be out there away from the world running. The coroner's report proclaimed the death to be due to a pre-existing heart condition, resulting in thickening of the left ventricular compartment. This scarring of the heart fits the sorts of heart defects that Dr. O'Keefe suggests are related to extreme exercise - Pheidippides cardiomyopathy as Peter McCullough describes it.
Next up we see a reflection on the death of Micah True, the legendary runner from Christopher McDougal's Born To Run, who unfortunately died last year at the young age of 58 whilst out on a routine training run. I was lucky enough to meet Micah last year, and he was a very friendly and unassuming individual. He ran because he loved to run, and had no agenda having had fame thrust upon him. He didn't care about arguments of barefoot vs shod running (for the record, he and the Tarahumara Indians do not run barefoot). He just loved to be out there away from the world running. The coroner's report proclaimed the death to be due to a pre-existing heart condition, resulting in thickening of the left ventricular compartment. This scarring of the heart fits the sorts of heart defects that Dr. O'Keefe suggests are related to extreme exercise - Pheidippides cardiomyopathy as Peter McCullough describes it.
{kind=link}
These data are quite compelling, but I really think that all it shows is that runners are not immune from such heart problems, not that runners are more likely to suffer from them. Almost to make that point for me, the next evidence that is used to make his point is a figure from an upcoming paper looking at 52,000 individuals (14,000 runners vs 38,000 non-runners), comparing the death rates of runners at various distances with those of non-runners. As Dr O'Keefe himself points out, the death rate is lower for runners than for non-runners. But the death rate is higher for longer distance runners than for shorter distance runners. But the important thing that seems to be glanced over is that this death rate is still lower than for non-runners. It is not clear whether this figure represents cardiac-related deaths or all deaths. If all deaths, then a large number of these deaths will be from problems like hyponatremia which account for the majority of deaths in marathons. This is actually a very important point, and I will be interested to read the paper to find out.
There are plenty of factors that have not been mentioned here. One that immediately comes to mind is diet, which can have a big effect on cardiac function. One possibility is that running longer distances results in a change in eating habits that is not conducive to a healthy heart (increased carbohydrate metabolism for instance). Another is the increased exposure of runners to environmental pollutants while out running. Another that has come up already is the level of training. It is possible that the increased prevalence of Pheidippides cardiomyopathy that these data may or may not indicate may not be due to the running itself, but instead due to factors associated with running. Or perhaps the runners with heart problems were not training as often as they should have been (obviously this was not the case for Micah). Or maybe these people just had heart problems, and happen to be runners? Either way, all of the other data still seem to suggest that runners suffer fewer deaths than non-runners.
My own view on this is that the cardiac problems associated with not running are far worse than those of running. The argument is that I shouldn't run so far because it is bad for me. What the data actually seem to show is that running long distances doesn't give me any extra benefit over running for an hour. But you know what? I don't run long distances to improve my health. That is just a nice added benefit. I love to be out there for a long time with my own thoughts, working through problems in my head, enjoying my surroundings, listening to music, listening to a good book, pushing myself in a race situation, running with friends, seeing some amazing scenery, visiting new places, and generally enjoy ingbeing out and about. Does running protect you against heart problems? To some degree it certainly appears so. Do I get any extra benefit from running for further? Maybe not. Am I immune from heart problems? No.
The argument at the end is that the right amount of exercise lies somewhere in the middle of a U-shaped curve. The couch potatoes at one end don't get any benefits, the extreme athletes at the other end also don't see any benefits, but it's the people in the middle doing a moderate amount of low pace running in the middle that are getting the benefits. But is that really the case? Sure I agree that "too much exercise is bad for you" - that's what "too much" means! But I disagree with what falls under the "too much" category. For somebody that has never run a day in their life, running a marathon is too much. For me, it's a weekly occurrence. The trick is to build things up slowly and allow your body to adapt. "Too much" is an ever-changing quantity, adaptable to the capabilities of the runner. Suggesting that everybody should run 2-3 miles at a 10 min/mile pace fails to account for the heterogeneity of people.
I don't claim that there is no merit to the claims that running extreme distances causes heart problems, but the evidence that I have seen so far is open to interpretation. Firstly, there are a large number of extreme athletes that haven't suffered from any form of heart defect (pulling Micah True and Jim Fix out as arguments against running ignores the much larger body of similar runners who haven't died young from heart conditions). As Dr. O'Keefe mentions towards the end, he has had a lot of negative correspondence from runners who refuse to believe these controversial claims. I have tried not to let my love of long-distance running bias my opinions too much on this (although obviously it has to some degree), and don't for one minute claim that there is any intentional misinformation on the part of O'Keefe and colleagues. However, I differ in my interpretation of what I have seen, and whilst I am not an expert in this specific field I do have a lot of experience in the interpretation of biological data (it is my job after all). My biggest worry is the way that the media sensationalises stories like this and encourage a more sedentary lifestyle (although this is clearly not what the authors intend). For now, I'm going to carry on running and enjoying myself, without worrying too much about this until I see some compelling evidence that I should not be doing what I love.
Note - I have edited two sections; slightly correcting a point that I made about the LeGerche paper (I have left the original there with strike-through so that you can see the context of the change), and added a paragraph that was missing from my initial post (highlighted in the text).
Note - I have edited two sections; slightly correcting a point that I made about the LeGerche paper (I have left the original there with strike-through so that you can see the context of the change), and added a paragraph that was missing from my initial post (highlighted in the text).
Nice post Sam, thanks for your take on this. I agree there is a fair amount of fairly subjective reading of the data being applied.
ReplyDeleteAs you point out in LeGerche et al all the cardiac parameters return to normal (and so seem to be simply an exercise response) and the supposed correlation of 'RV dysfunction' with duration of exercise is pretty weak. The 'baseline' is pretty hard to interpret as well without a matched non-athelete group, given that all these people have already got considerable training history.
In the way the paper has been cited it seems there is a rather simplistic (but sadly widespread) misinterpretation of the 'biomarker' analysis without considering the biological relevance and context of the person being sampled.
Fortunately, for the imaging LeGerche do point out 'However, care must be taken when drawing analogies...Such prognostic implications should not be extrapolated to the healthy cohort of athletes presented here.'
You're absolutely right Nick, and it certainly seems that the authors of the LeGerche paper were careful to distance themselves from any media sensationalism (not that it helped of course). I went into a bit more detail of the methodological problems in my previous post, but I thought this one was long and rambling enough as it was! But I couldn't help but get the feeling that this TED talk was aiming to actually court the controversy, and some of the more speculative claims seemed to be declared with absolute certainty. What do other people think?
ReplyDeleteGreat read Sam. What gets me with all these "running is bad for you" articles is that they never consider the quality of life running gives. Maybe it will knock 10 years off your life so rather than living to 90 you will drop dead at 80. But what matters in your final days isn't how long you've lived but how well you've lived. If those 80 years are full of energy with much done and achieved I for one would be happy to pass up on the extra 10 years I might have had if I'd spent more time in front of the TV.
ReplyDeleteReally great read - thank you for setting it out so well and getting to grips with a decent amount of research on the issue! As an econometrician (I keep it well hidden...) I am delighted to see the myths busted especially correlation does not equal causation. Poor sampling and anecdote shouldn't be used as evidence either. There is also the much overlooked selection bias for longer runners - which has endogeniety issues that are rarely considered in the research.
ReplyDeleteAnd you're right - it's my experience that many people start running for the health benefits, but no one runs 100 miles through the mountains for their health - it becomes about the experience and the fun of it. Jen
I'm sure you're right that one of the aims was to generate media attention - unfortunately it's all too easy to pull some data out of context from papers and create a sensationalist story (which then persists - look at the length of time that the MMR nonsense had an impact on vaccination rates). Once people start quoting anecdotal evidence it kind of rings alarm bells on their credibility, so its very good that posts like yours highlight the inconsistent arguments.
ReplyDeleteSpecifically on ultrarunning, despite the rise in popularity I would be amazed if there is any current study that has a sample size to be powered to detect a detrimental effect once data is corrected for BMI, age, smoking etc (from your research on the diverse group of people on centurion events I guess you'd be able to make some estimate).
I enjoyed your article. I would like to make a few points regarding my personal beliefs which I think many others may agree with.
ReplyDelete-I run because it makes me happy not to live longer. I am an oncologist and see people die every day. In my opinion life is about enjoying the time you have - for me a part of that is running.
-I ran in college. When I stopped running I started drinking beer and chewing tobacco for 10 years. I started running again and stopped drinking and chewing. I think running makes people drink less alcohol, smoke less tobacco, and eat healthier.
-Although it seems simple on the outside - isolating the variable of running proves to be difficult. Using the CAC level as an endpoint is worthless in my opinion. It's an indicator of health but not a direct measure. Further, the data used to develop the CAC score did not distinguish runners from non runners. This is important because it us unknown if coronary plaque stability is the same in runners vs. non runners.
-The only way to address the route of the problem is to have a large scale randomized controlled trial with runners and non runners over a long period of time and plot it on a Kaplan Meier survival curve. Then do a subset analysis of causes of death. I think isolating variables like smoking history would be a mistake because not smoking can have a causal relationship with running as was the case for me and likely many others.
- If you love to run, go run and be happy.
I have been a runner since I could "walk". I am 40, still running recreationally with my dogs and my kids in tow about 3 miles several times a week. I have trained and participated in 1/2 marathon training and races. Plus I road bike, hike, rollerblade, nordic ski, P90X several times a week, eat a gluten free diet, no smoking, low alcohol intake, etc. I do what I want and how much of what I want to do. Running a marathon has never been an interest to me, mainly because I have no interest in running THAT much; and two I don't have the time for it because of my life and other interests that compete with that kind of training schedule.
ReplyDeleteI think that there are many variables when looking at someone's heart health. But I also have known for a long time that there are many strains that can be put on the heart, regardless of how "fit" you are. The only way to really track this properly is to take all the marathoners and ultra runners and look at their hearts as well as get feedback on what their diet is like.
All that aside though, I still think that it is a moot point. People are going to do what they want to do even if it means an earlier death or deterioration of their heart or break down of their joints, etc. We can see these same tendencies in people on the other end of the fitness spectrum.
Bottom line, I think that participating in what I like to call "extreme" sports (anything that goes above and beyond what most people would consider moderate), boils down to a personality thing. Some people just like to push themselves to the very limit of endurance. Even when death faces them in the eyes they still carry on. And they love every minute of it. Everyone has different ways of experiencing what life has to offer. Some like to take things at a moderate pace and others like to push limits. Like the above person wrote, it's all about doing what you love and doing how you like to do it. But I also think that it is wise to exercise prudence and some good judgement and listen to your body.